Introduction to Cardiology billing
Managing cardiology billing requires precise coding knowledge and attention to detail. This comprehensive guide covers every major code you will encounter in a cardiology practice, from routine visits to complex procedures.
Evaluation and Management (E/M) Services
Office/Outpatient Visits New Patients
• 99201: Level 1 (Discontinued as of 2021)
• 99202: Level 2 Straightforward medical decision making (MDM)
• 99203: Level 3 Low MDM
• 99204: Level 4 Moderate MDM
• 99205: Level 5 High MDM• 99201: Level 1 (Discontinued as of 2021)
• 99202: Level 2 Straightforward medical decision making (MDM)
• 99203: Level 3 Low MDM
• 99204: Level 4 Moderate MDM
• 99205: Level 5 High MDM
Office/Outpatient Visits Established Patients
• 99211: Level 1 Minimal presenting problems
• 99212: Level 2 Straightforward MDM
• 99213: Level 3 Low MDM
• 99214: Level 4 Moderate MDM
• 99215: Level 5 High MDM
Hospital Services
• 99221 to 99223: Initial hospital care
• 99231 to 99233: Subsequent hospital care
• 99238 to 99239: Hospital discharge services
• 99291 to 99292: Critical care services
Diagnostic Testing Codes
Electrocardiography
• 93000: ECG with interpretation and report
• 93005: ECG tracing only
• 93010: ECG interpretation and report only
• 93040: Rhythm ECG with interpretation
• 93041: Rhythm ECG tracing only
• 93042: Rhythm ECG interpretation only
Holter Monitoring
• 93224: 24 hour Holter monitoring (complete)
• 93225: Hookup and recording
• 93226: Scanning analysis with report
• 93227: Physician review and interpretation
• 93228: Mobile cardiac telemetry up to 30 days
• 93229: Technical support for mobile cardiac telemetry
Echocardiography
• 93303: Echo, congenital
• 93304: Echo, congenital follow up
• 93306: Echo complete with spectral and color flow
• 93307: Echo without spectral and color flow
• 93308: Echo follow up
• 93312: TEE probe placement and imaging
• 93315: TEE for congenital anomalies
• 93318: TEE for monitoring purposes
Stress Testing
• 93350: Stress echo
• 93351: Stress echo with contrast
• 93015: Cardiovascular stress test complete
• 93016: Physician supervision only
• 93017: Tracing only
• 93018: Interpretation and report only
Cardiac Catheterization
Diagnostic Procedures
• 93451: Right heart catheterization
• 93452: Left heart catheterization
• 93453: Combined right and left heart catheterization
• 93454: Coronary angiography
• 93455: Coronary angiography with bypass grafts
• 93456: Right heart catheterization with coronary angiography
• 93457: Right heart catheterization with coronary angiography and bypass grafts
• 93458: Left heart catheterization with coronary angiography
• 93459: Left heart catheterization with coronary angiography and bypass grafts
• 93460: Right and left heart catheterization with coronary angiography
• 93461: Right and left heart catheterization with coronary angiography and bypass grafts
Interventional Procedures
Coronary Interventions
• 92920: Percutaneous transluminal coronary angioplasty (PTCA) single
• 92921: Each additional vessel PTCA
• 92924: PTCA with atherectomy single vessel
• 92925: Each additional vessel with atherectomy
• 92928: PCI with stent placement single vessel
• 92929: Each additional vessel with stent
• 92933: PCI with atherectomy and stent single vessel
• 92934: Each additional vessel with atherectomy and stent
• 92937: PCI for chronic total occlusion
• 92938: Each additional chronic total occlusion
• 92943: PCI for chronic total occlusion with atherectomy
• 92944: Each additional vessel chronic total occlusion with atherectomy
Structural Heart Procedures
• 93580: ASD closure device
• 93581: VSD closure device
• 93582: PFO closure device
• 93583: PVLS closure device
• 93590: Aortic valve replacement percutaneous
• 93591: Aortic valve replacement transapical
• 93592: Additional valve replacement
Common ICD 10 Codes
Hypertensive Diseases
• I10: Essential hypertension
• I11.0: Hypertensive heart disease with heart failure
• I11.9: Hypertensive heart disease without heart failure
• I12.0: Hypertensive CKD with stage 5 or ESRD
• I12.9: Hypertensive CKD without heart failure
• I13.0: Hypertensive heart and CKD with heart failure and stage 1 to 4 CKD
• I13.2: Hypertensive heart and CKD with heart failure and stage 5 CKD or ESRD
Ischemic Heart Disease
• I20.0: Unstable angina
• I20.1: Angina pectoris with documented spasm
• I20.8: Other forms of angina pectoris
• I20.9: Angina pectoris unspecified
• I21.0 to I21.4: Acute myocardial infarction (specific types)
• I21.9: Acute myocardial infarction unspecified
• I25.10: Atherosclerotic heart disease without angina
• I25.110: ASHD with unstable angina
• I25.111: ASHD with angina pectoris with documented spasm
• I25.118: ASHD with other forms of angina
• I25.119: ASHD with unspecified angina
Arrhythmias
• I47.0: Re entry ventricular arrhythmia
• I47.1: Supraventricular tachycardia
• I47.2: Ventricular tachycardia
• I48.0: Paroxysmal atrial fibrillation
• I48.1: Persistent atrial fibrillation
• I48.2: Chronic atrial fibrillation
• I48.91: Unspecified atrial fibrillation
• I49.01: Ventricular fibrillation
• I49.02: Ventricular flutter
• I49.1: Atrial premature depolarization
• I49.2: Junctional premature depolarization
• I49.3: Ventricular premature depolarization
Heart Failure
• I50.1: Left ventricular failure
• I50.20: Unspecified systolic heart failure
• I50.21: Acute systolic heart failure
• I50.22: Chronic systolic heart failure
• I50.23: Acute on chronic systolic heart failure
• I50.30: Unspecified diastolic heart failure
• I50.31: Acute diastolic heart failure
• I50.32: Chronic diastolic heart failure
• I50.33: Acute on chronic diastolic heart failure
• I50.40: Unspecified combined systolic and diastolic heart failure
• I50.41: Acute combined systolic and diastolic heart failure
• I50.42: Chronic combined systolic and diastolic heart failure
• I50.43: Acute on chronic combined systolic and diastolic heart failure
• I50.9: Heart failure unspecified
Important Modifiers
• 25: Significant, separately identifiable E/M service
• 26: Professional component
• TC: Technical component
• 59: Distinct procedural service
• 22: Increased procedural services
• 52: Reduced services
• 53: Discontinued procedure
• 76: Repeat procedure by same physician
• 77: Repeat procedure by another physician
• 78: Return to OR for related procedure
• 79: Unrelated procedure during postoperative period
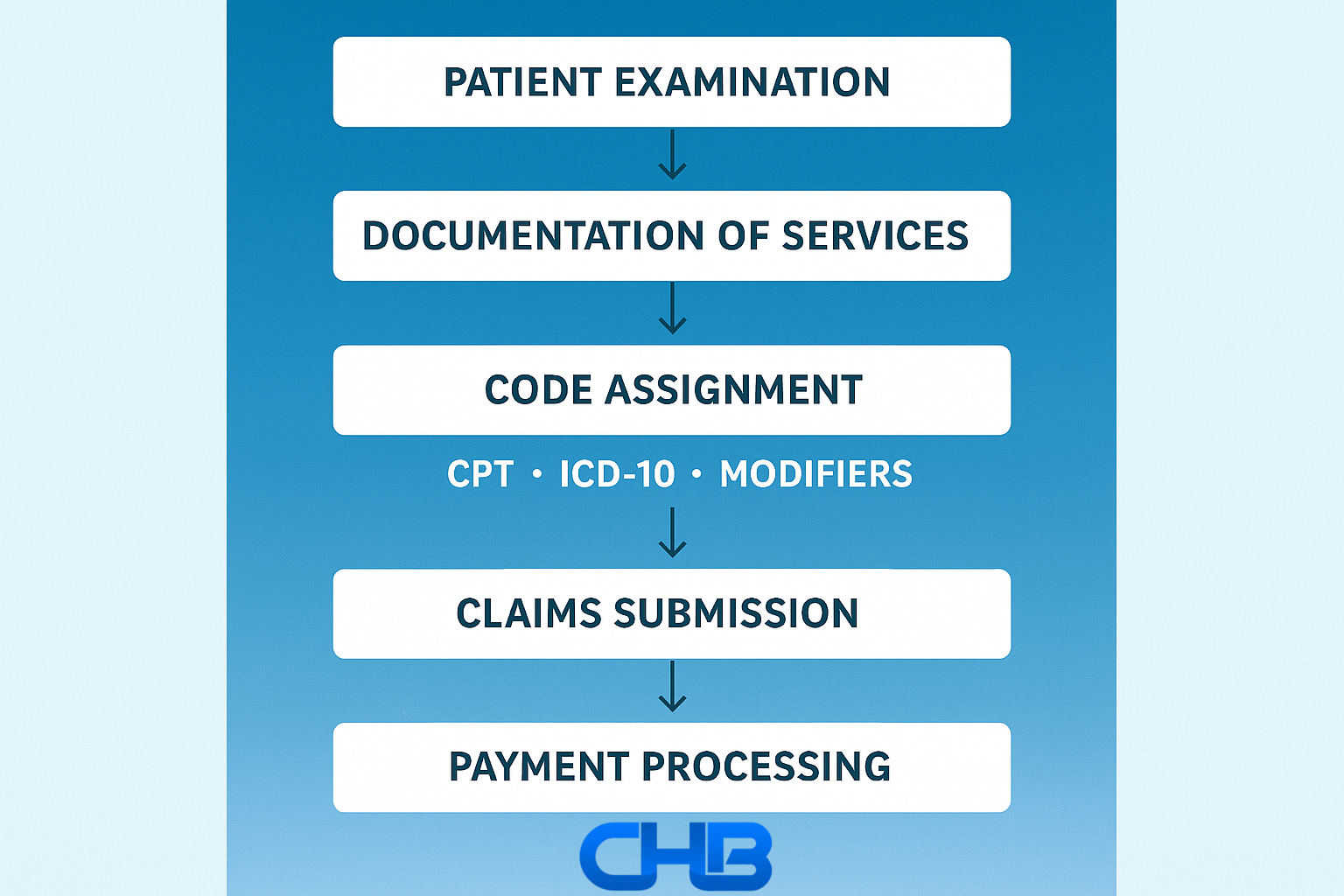
Documentation Requirements
Each procedure requires specific documentation elements for proper reimbursement. Key components include:
• Medical necessity
• Patient history and symptoms
• Physical examination findings
• Test results and interpretation
• Medical decision making
• Plan of care
• Time spent (when applicable)
• Risk factors and comorbidities
Billing Tips for Maximum Reimbursement
• Always verify insurance coverage and prior authorization requirements
• Document medical necessity thoroughly
• Use the most specific diagnosis codes available
• Include appropriate modifiers
• Submit clean claims within timely filing deadlines
• Monitor denials and appeal when appropriate
• Stay current with coding updates and changes
• Perform regular internal audits
• Maintain compliance with documentation requirements
Outsourcing your billing to a specialized medical billing company ensures your codes are thoroughly reviewed for accuracy, helping prevent denials and maximize reimbursements. Though we are not a coding company, we meticulously verify the correctness of submitted codes. Consider using certified coders for complex cases.
FAQ:
Q: How do I use the 25 modifier correctly for cardiology?
A: Use it when billing for an E/M service with a procedure on the same day. For example, if a cardiologist evaluates chest pain and performs an ECG, both services are billable but the E/M code needs the 25 modifier.
Q: What is the difference between the 26 and TC modifiers?
A: The 26 modifier is for the professional component (eg interpretation of an ECG), while TC covers the technical component (eg use of the ECG machine). Use both if you are billing separately for professional and technical services.
Q: How do cardiology practices reduce claim denials?
A: Keep documentation thorough, verify insurance before procedures, use appropriate modifiers, and monitor denial trends. Using an EHR with built in coding tools also helps catch errors early.
Q: What procedures require prior authorization in cardiology?
A: High cost diagnostic procedures such as nuclear stress tests, cardiac MRIs, and some catheterization procedures often require prior approval from the payer.
Q: How can I handle denied cardiology claims efficiently?
A: Investigate the reason for denial, correct the errors, and resubmit the claim. Appeal if necessary by providing supporting documentation such as medical necessity notes.
Read More: